A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
Innhold levert av The Physician Assistant Life | Smarty PANCE. Alt podcastinnhold, inkludert episoder, grafikk og podcastbeskrivelser, lastes opp og leveres direkte av The Physician Assistant Life | Smarty PANCE eller deres podcastplattformpartner. Hvis du tror at noen bruker det opphavsrettsbeskyttede verket ditt uten din tillatelse, kan du følge prosessen skissert her https://no.player.fm/legal.
Lik The Audio PANCE and PANRE Physician Assistant Board Review Podcast
Montgomery & Company (MoCo) is a weekly podcast and radio show hosted by two-time WNBA Champion and Co-Owner/Vice President of the Atlanta Dream, Renee Montgomery, in partnership with WABE Atlanta. Both insightful and compelling, MoCo features interviews with some of the world’s top athletes, entertainers, and innovators as well as roundtable discussions with Renee’s colleagues, friends, and family, about sports, culture and building generational wealth. Montgomery & Company: Sports, Cultu ...
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Join host and Harvard Business School Online Creative Director Chris Linnane as he sits down with HBS faculty to discuss business education in a way that’s both entertaining and insightful. The Parlor Room is your key to breaking down academic theory without sacrificing depth—all while gaining practical takeaways for navigating the business world.
…
continue reading
How can business help solve society’s biggest challenges? Welcome to Series 3 of Take on Tomorrow, the award-winning podcast from PwC that examines the biggest problems facing society and the role business can—and should—play in solving them. This series, we’re welcoming broadcaster and journalist Femi Oke to the show. She joins podcaster and journalist Lizzie O’Leary, and together with industry innovators, tech trailblazers and visionary leaders from around the globe, they’ll explore timely ...
…
continue reading
The traditional enterprise go-to-market motion is undergoing a transformational shift. B2B buyers are more sophisticated than ever, and operational efficiency is a key focus for every organization. One key function possesses a unique opportunity to shape the future of revenue generation: enablement. On this podcast, we’re bringing you the secrets, strategies, and tactics that successful enablement leaders are using to drive meaningful impact. The Enablement Edge is the go-to resource for sal ...
…
continue reading
AnthroPod is produced by the Society for Cultural Anthropology. In each episode, we explore what anthropology teaches us about the world and people around us.
…
continue reading
From the stuff your mother never told you, to the stuff your doctor never learned, On Health features taboo-busting conversations that demystify and de-stigmatize our bodies, all while bridging the gap between conventional medicine and wellness. Join Yale-trained MD & midwife Aviva Romm and her line-up of expert guests as they discuss everything from periods to menopause, sex to reproductive health politics, and motherhood to mental health. Each week, Dr. Romm will be exploring the science a ...
…
continue reading
New episode every Wednesday! Join the Barbell Shrugged crew in conversations about fitness, training, and frequent interviews w/ CrossFit Games athletes!
…
continue reading
I Tyngre Radio snackas det om styrketräning. Punkt. Värdar är Alex Danielsson och Andreas Guiance.
…
continue reading
Player FM - Podcast-app
Gå frakoblet med Player FM -appen!
Gå frakoblet med Player FM -appen!

))
Podcast Episode 107: This vs. That – PANCE Blueprint Comparisons You Need to Know (Part 1)
Manage episode 374308962 series 97199
Innhold levert av The Physician Assistant Life | Smarty PANCE. Alt podcastinnhold, inkludert episoder, grafikk og podcastbeskrivelser, lastes opp og leveres direkte av The Physician Assistant Life | Smarty PANCE eller deres podcastplattformpartner. Hvis du tror at noen bruker det opphavsrettsbeskyttede verket ditt uten din tillatelse, kan du følge prosessen skissert her https://no.player.fm/legal.
Listen to Podcast Episode 107: This vs. That – PANCE Blueprint Comparisons You Need to Know (Episode 1)
In today’s session, we will be discussing five questions related to PANCE/PANRE Blueprint topics. These questions will cover similar presentations and crucial comparisons that are important for you to know. These topics are often used by PANCE/PANRE test question writers, so it’s essential to learn how to differentiate between them. This is the first part (episode 1) of a series.
If you can’t see the audio player, click here to listen to the full episode.
Links from today’s episode:
- Sign up for our new PANCE and PANRE Test-Taking Masterclass.
- Check out my first blog in our “This vs. That” Blueprint series: The PANCE Blueprint Showdown: Crohn’s Disease vs. Ulcerative Colitis.
- Want a question of the day that covers the Blueprint – ALL of it? Sign up for the Entire Blueprint Email Series.
- Follow Smarty PANCE and The Daily PANCE Blueprint on Instagram and Facebook for more daily questions.
- Join the Smarty PANCE Member’s Community, then sign up for a study group to get updates about upcoming webinars.
I hope you enjoy this free audio component of the examination portion of this site. Smarty PANCE includes over 2,000 interactive board review questions, along with flashcards, ReelDx cases, integrated Picmonics, and lessons covering every blueprint topic available to all Smarty PANCE members.
- You can download and listen to past FREE episodes here, on iTunes, Spotify, Google Podcasts, Stitcher, Amazon Music, and all podcasting apps.
- You can listen to all the latest episodes, take interactive quizzes, and download more resources on each episode page.
Interactive exam to complement today’s podcast
1. A 32-year-old woman presents with a 6-month history of loose bowel movements, approximately eight per day. Blood has been present in many of them. She has lost 30 pounds. For the past 6 weeks, she has had intermittent fever. She has had no previous gastrointestinal (GI) problems, and there is no family history of GI problems. On examination, the patient looks ill. Her blood pressure is 130/ 70 mm Hg. Her pulse is 108 beats/ minute and regular. There is generalized abdominal tenderness with no rebound. A sigmoidoscopy reveals a friable rectal mucosa with multiple bleeding points. Which of the following is the most likely diagnosis?
A) Crohn’s Disease
B) Ulcerative Colitis
C) Infectious Colitis
D) Irritable Bowel Syndrome (IBS)
E) Ischemic Colitis
Answer and topic summary
The answer is B) Ulcerative Colitis
The patient’s symptoms of chronic bloody diarrhea, weight loss, fever, and the sigmoidoscopy findings of a friable rectal mucosa with multiple bleeding points are consistent with a diagnosis of ulcerative colitis (UC), which is a form of inflammatory bowel disease (IBD). UC typically involves the rectum and may extend proximally to involve other parts of the colon.
Incorrect answers:
A) Crohn’s Disease: This is another type of IBD. However, Crohn’s usually presents with non-bloody diarrhea, abdominal pain, and may involve any part of the GI tract from mouth to anus, often with skip lesions. In this case, the bloody diarrhea and the findings on sigmoidoscopy are more indicative of ulcerative colitis.
C) Infectious Colitis: Although infectious causes can lead to similar symptoms, the duration of this patient’s symptoms (6 months) is much longer than typically seen with infectious colitis. Additionally, fever is less common in infectious colitis.
D) Irritable Bowel Syndrome (IBS): IBS is a functional GI disorder characterized by abdominal pain with a change in bowel habit. It does not cause weight loss, fever, or bloody stools.
E) Ischemic Colitis: This typically presents acutely in older patients or those with vascular risk factors. The clinical presentation often includes abrupt onset of abdominal pain and bloody diarrhea. The duration and pattern of symptoms in this patient are more consistent with IBD.
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint GI and Nutrition ⇒ Colorectal disorders ⇒ Inflammatory bowel disease
2. A 27-year-old female presents to the emergency department with a 3-day history of a widespread painful rash. She reports having started a new medication for her seizures 1 week ago. On examination, you note erythematous macules that are coalescing into large areas of epidermal detachment. The mucous membranes of her mouth, eyes, and genital region are also affected, and the skin involvement covers more than 30% of her body surface area. A skin biopsy reveals full-thickness epidermal necrosis. Based on her presentation and the medication history, which of the following diagnoses is she most likely suffering from, and which medication most likely contributed to this condition?
A) Erythema multiforme major secondary to Levetiracetam (Keppra)
B) Toxic Epidermal Necrolysis (TEN) secondary to Carbamazepine
C) Stevens-Johnson syndrome (SJS) secondary to Metformin
D) Acute generalized exanthematous pustulosis secondary to Lisinopril
E) Stevens-Johnson syndrome (SJS) secondary to Atorvastatin
Answer and topic summary
The answer is B) Toxic Epidermal Necrolysis (TEN) secondary to Carbamazepine
The patient’s presentation with widespread epidermal necrosis, mucous membrane involvement, and skin detachment affecting more than 30% of her body surface area is suggestive of Toxic Epidermal Necrolysis (TEN). SJS and TEN are considered a spectrum of the same disease, with SJS affecting less than 10% of body surface area, SJS-TEN overlap affecting 10-30%, and TEN affecting more than 30%. The diagnosis can be confirmed by biopsy (showing necrotic epithelium) if clinical characteristics (eg, target lesions progressing to bullae, ocular and mucous membrane involvement, Nikolsky sign, desquamation in sheets) are inconclusive. Immediate discontinuation of the offending drug is paramount. Patients with TEN often require transfer to a burn unit or an intensive care unit for supportive care. Fluid and electrolyte balance, pain control, and prevention of secondary infections are critical. Immunomodulatory agents like IVIG (intravenous immunoglobulin) or cyclosporine may be considered, but their efficacy is still under debate.
Option A: Erythema multiforme major: Presents with targetoid lesions and is less severe than SJS and TEN. Levetiracetam is not strongly associated with SJS or TEN.
Option D: Acute generalized exanthematous pustulosis is an extensive formation of nonfollicular sterile pustules on erythematous background combined with fever and peripheral blood leukocytosis. This uncommon eruption is most often an allergic reaction because of drugs such as aminopenicillins and sulfonamides inter alia.
A good way to remember the body surface area affected in TEN is “T hree x T en = T hirty percent in Toxic Epidermal Necrolysis
The distinction between SJS, SJS/TEN overlap, and TEN is based on the type of lesions and the amount of the body surface area with blisters and erosions
- Blisters and erosions cover between 3% and 10% of the body in SJS
- 11–30% in SJS/TEN overlap
- over 30% in TEN
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Dermatology ⇒ Desquamation ⇒ Toxic epidermal necrolysis and Stevens-Johnson syndrome
3. A 32-year-old male presents to his primary care physician complaining of persistent fatigue, unintentional weight loss over the past 3 months, and a painless swelling in the left side of his neck. On examination, there is a non-tender, rubbery 3cm lymphadenopathy in the left cervical region. A subsequent excisional biopsy of the node is performed, and microscopy reveals large atypical cells with abundant cytoplasm and bilobed nuclei, reminiscent of an “owl’s eye” appearance. What is the most likely diagnosis?
A) Acute lymphoblastic leukemia (ALL)
B) Non-Hodgkin’s Lymphoma
C) Burkitt’s lymphoma
D) Hodgkin’s Lymphoma
E) Chronic lymphocytic leukemia (CLL)
Answer and topic summary
The answer is D) Hodgkin’s Lymphoma
The patient’s clinical presentation with painless cervical lymphadenopathy and constitutional symptoms, coupled with the histological finding of large cells bearing the “owl’s eye” appearance (Reed-Sternberg cells), is characteristic of Hodgkin’s Lymphoma. Hodkin’s lymphoma is the most common type of lymphoma and usually presents as a solitary cervical lymph node that has been there for > 30 days. It is commonly manifested with painless cervical adenopathy; there may be splenomegaly or enlargement of other immune tissue, fever, weight loss, fatigue, or night sweats. Upper body lymph nodes are the most common. Diagnosis is based on clinical presentation and confirmed by an excisional biopsy of an involved lymph node. Histology often reveals the pathognomonic Reed-Sternberg cells, which have bilobed nuclei. A chest radiograph should be obtained to search for mediastinal adenopathy. Treatment for Hodgkin’s Lymphoma depends on the stage of the disease and typically involves a combination of chemotherapy, most commonly the ABVD regimen (Adriamycin, Bleomycin, Vinblastine, Dacarbazine). Radiation therapy might be added, especially for localized disease.
Answer Choices Explanations:
A) Acute lymphoblastic leukemia (ALL): Affects mainly children and presents with bone marrow failure symptoms.
B) Non-Hodgkin’s Lymphoma: A group of lymphoid malignancies. Reed-Sternberg cells distinguish Hodgkin’s Lymphoma from Non-Hodgkin’s types.
C) Burkitt’s lymphoma: Fast-growing non-Hodgkin’s lymphoma linked to the Epstein-Barr virus. Exhibits a “starry sky” appearance on microscopy.
E) Chronic lymphocytic leukemia (CLL): A malignancy of mature B cells in older adults. Increased lymphocyte count and smudge cells on a peripheral blood smear.
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Hematology ⇒ Neoplasms, premalignancies, and malignancies ⇒ Lymphoma (ReelDx + Lecture)
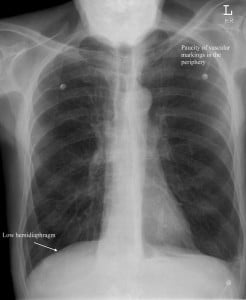
4. A 65-year-old male presents to your office complaining of fatigue and shortness of breath with exertion. The patient reports minimal cough. On physical exam, you note a thin, barrel-chested man with decreased heart and breath sounds, pursed-lip breathing, end-expiratory wheezing, and scattered rhonchi. Chest X-ray reveals a flattened diaphragm, hyperinflation, and a small, thin-appearing heart. PFTs show a decreased FEV1 / FVC ratio.
A) Asthma
B) Chronic bronchitis
C) Emphysema
D) Pulmonary fibrosis
E) Bronchiectasis
Answer and topic summary
The answer is C. Emphysema
The patient’s presentation of shortness of breath with exertion, barrel-chested appearance, pursed-lip breathing, findings on chest X-ray (e.g., flattened diaphragm, hyperinflation, and a small heart), and pulmonary function test results all align with the diagnosis of emphysema.
Emphysema is a lung disease that causes shortness of breath. It is one of the two main conditions that make up chronic obstructive pulmonary disease (COPD). The other condition is chronic bronchitis.
In emphysema, the air sacs (alveoli) in the lungs are damaged. Over time, the inner walls of the air sacs weaken and rupture — creating larger air spaces instead of many small ones. This reduces the surface area of the lungs and, in turn, the amount of oxygen that reaches your bloodstream.
The main cause of emphysema is cigarette smoking. Other causes include air pollution and chemical fumes. A small percentage of cases are caused by a familial or genetic disorder, alpha-1-antitrypsin deficiency.
- The body’s natural response to ↓ lung function is chronic hyperventilation = Pink Puffers! CO2 Retainers – the body must increase ventilation to blow off CO2
- Minimal cough (compared to chronic bronchitis), quiet lungs
- Minimal sputum (compared to chronic bronchitis)
- Thin, underweight, and barrel chest
Answer Choices Explanations:
A) Asthma: An obstructive lung disease that is reversible and is marked by bronchoconstriction. It typically presents with episodes of wheezing triggered by factors such as allergens, exercise, or infections.
B) Chronic bronchitis: Defined by a productive cough for 3 consecutive months in 2 successive years. It’s a subtype of chronic obstructive pulmonary disease (COPD), with its main causative factor being smoking. The primary concern is mucus production, as opposed to the alveolar wall destruction seen in emphysema.
D) Pulmonary fibrosis: Represents a set of disorders causing scarring of the lung tissue, leading to a restrictive lung disease pattern. Symptoms might include a dry cough, finger clubbing, and inspiratory crackles upon examination.
E) Bronchiectasis: It is marked by the chronic dilation of bronchi or bronchioles due to repeated infections and inflammation. Patients often have a chronic cough and produce significant amounts of sputum.
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Pulmonary ⇒ Chronic obstructive pulmonary diseases ⇒ Emphysema
Also covered as part of the Internal Medicine EOR, Family Medicine EOR, and General Surgery EOR topic lists
5. A 68-year-old woman presents to the emergency department with chest pain that started 5 hours ago. She describes the pain as a heavy pressure radiating to her left arm. It began at rest and has persisted. She has a history of hypertension and diabetes mellitus. An ECG shows ST-segment depressions in leads II, III, and aVF. Troponin I levels are elevated at 0.55 ng/mL (normal: <0.04 ng/mL). Which of the following is the most likely diagnosis?
A) Stable angina
B) Unstable angina
C) Non-ST segment elevation myocardial infarction (NSTEMI)
D) ST-segment elevation myocardial infarction (STEMI)
E) Prinzmetal angina
Answer and topic summary
The answer is C) Non-ST segment elevation myocardial infarction (NSTEMI)
This patient’s presentation with chest pain at rest, ST-segment depressions on ECG, and elevated troponin I levels are consistent with NSTEMI. NSTEMI is characterized by myocardial ischemia severe enough to result in myocyte injury and elevated cardiac biomarkers but not sufficient to cause ST-segment elevation on ECG.
NSTEMI is diagnosed clinically with supporting findings from ECG changes, especially ST-segment depressions or T-wave inversions, and elevated cardiac biomarkers (troponins or CK-MB). Elevated troponins, in particular, differentiate NSTEMI from unstable angina.
Immediate management includes antiplatelet agents (e.g., aspirin, clopidogrel), anticoagulation (e.g., heparin or enoxaparin), and nitrates for symptom relief. A coronary angiography, followed by possible revascularization (percutaneous coronary intervention or coronary artery bypass grafting), might be required based on risk assessment.
Answer Choices Explanations:
A) Stable angina: Characterized by predictable chest pain or discomfort with exertion or stress, which is relieved by rest or nitroglycerin.
B) Unstable angina: Presents as chest pain at rest, new-onset angina, or angina that is more frequent, longer in duration, or not relieved by rest/nitroglycerin. Crucially, cardiac biomarkers (e.g., troponins) remain normal, differentiating it from NSTEMI.
D) ST-segment elevation myocardial infarction (STEMI): Acute myocardial infarction characterized by ST-segment elevation on ECG. Requires immediate reperfusion therapy.
E) Prinzmetal angina: Caused by coronary artery spasm leading to transient ST-segment elevation. Pain typically occurs at rest, often in the early morning hours.
Smarty PANCE Content Blueprint Review:
PANCE Blueprint Cardiology => Coronary Heart Disease (PEARLS) => Non-ST-Segment Elevation MI (NSTEMI) ReelDx
This podcast is available on every device!
You can download and listen to past FREE episodes here, on iTunes, Spotify, Google Podcasts, Stitcher, Amazon Music, and all podcasting apps.
Download Interactive Content Blueprint Checklists for the PANCE, PANRE, EOR, and PANRE-LA
Follow this link to download your FREE copy of the PANCE/PANRE/EOR Content Blueprint Checklists.
Print it up and start crossing out the topics you understand, marking the ones you don’t, and making notes of key terms you should remember. The PDF version is interactive and linked directly to the individual lessons on Smarty PANCE.
Smarty PANCE is not sponsored or endorsed by, or affiliated with, the National Commission on Certification of Physician Assistants.
The post Podcast Episode 107: This vs. That – PANCE Blueprint Comparisons You Need to Know (Part 1) appeared first on The Audio PANCE and PANRE.
68 episoder
Podcast Episode 107: This vs. That – PANCE Blueprint Comparisons You Need to Know (Part 1)
The Audio PANCE and PANRE Physician Assistant Board Review Podcast
Manage episode 374308962 series 97199
Innhold levert av The Physician Assistant Life | Smarty PANCE. Alt podcastinnhold, inkludert episoder, grafikk og podcastbeskrivelser, lastes opp og leveres direkte av The Physician Assistant Life | Smarty PANCE eller deres podcastplattformpartner. Hvis du tror at noen bruker det opphavsrettsbeskyttede verket ditt uten din tillatelse, kan du følge prosessen skissert her https://no.player.fm/legal.
Listen to Podcast Episode 107: This vs. That – PANCE Blueprint Comparisons You Need to Know (Episode 1)
In today’s session, we will be discussing five questions related to PANCE/PANRE Blueprint topics. These questions will cover similar presentations and crucial comparisons that are important for you to know. These topics are often used by PANCE/PANRE test question writers, so it’s essential to learn how to differentiate between them. This is the first part (episode 1) of a series.
If you can’t see the audio player, click here to listen to the full episode.
Links from today’s episode:
- Sign up for our new PANCE and PANRE Test-Taking Masterclass.
- Check out my first blog in our “This vs. That” Blueprint series: The PANCE Blueprint Showdown: Crohn’s Disease vs. Ulcerative Colitis.
- Want a question of the day that covers the Blueprint – ALL of it? Sign up for the Entire Blueprint Email Series.
- Follow Smarty PANCE and The Daily PANCE Blueprint on Instagram and Facebook for more daily questions.
- Join the Smarty PANCE Member’s Community, then sign up for a study group to get updates about upcoming webinars.
I hope you enjoy this free audio component of the examination portion of this site. Smarty PANCE includes over 2,000 interactive board review questions, along with flashcards, ReelDx cases, integrated Picmonics, and lessons covering every blueprint topic available to all Smarty PANCE members.
- You can download and listen to past FREE episodes here, on iTunes, Spotify, Google Podcasts, Stitcher, Amazon Music, and all podcasting apps.
- You can listen to all the latest episodes, take interactive quizzes, and download more resources on each episode page.
Interactive exam to complement today’s podcast
1. A 32-year-old woman presents with a 6-month history of loose bowel movements, approximately eight per day. Blood has been present in many of them. She has lost 30 pounds. For the past 6 weeks, she has had intermittent fever. She has had no previous gastrointestinal (GI) problems, and there is no family history of GI problems. On examination, the patient looks ill. Her blood pressure is 130/ 70 mm Hg. Her pulse is 108 beats/ minute and regular. There is generalized abdominal tenderness with no rebound. A sigmoidoscopy reveals a friable rectal mucosa with multiple bleeding points. Which of the following is the most likely diagnosis?
A) Crohn’s Disease
B) Ulcerative Colitis
C) Infectious Colitis
D) Irritable Bowel Syndrome (IBS)
E) Ischemic Colitis
Answer and topic summary
The answer is B) Ulcerative Colitis
The patient’s symptoms of chronic bloody diarrhea, weight loss, fever, and the sigmoidoscopy findings of a friable rectal mucosa with multiple bleeding points are consistent with a diagnosis of ulcerative colitis (UC), which is a form of inflammatory bowel disease (IBD). UC typically involves the rectum and may extend proximally to involve other parts of the colon.
Incorrect answers:
A) Crohn’s Disease: This is another type of IBD. However, Crohn’s usually presents with non-bloody diarrhea, abdominal pain, and may involve any part of the GI tract from mouth to anus, often with skip lesions. In this case, the bloody diarrhea and the findings on sigmoidoscopy are more indicative of ulcerative colitis.
C) Infectious Colitis: Although infectious causes can lead to similar symptoms, the duration of this patient’s symptoms (6 months) is much longer than typically seen with infectious colitis. Additionally, fever is less common in infectious colitis.
D) Irritable Bowel Syndrome (IBS): IBS is a functional GI disorder characterized by abdominal pain with a change in bowel habit. It does not cause weight loss, fever, or bloody stools.
E) Ischemic Colitis: This typically presents acutely in older patients or those with vascular risk factors. The clinical presentation often includes abrupt onset of abdominal pain and bloody diarrhea. The duration and pattern of symptoms in this patient are more consistent with IBD.
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint GI and Nutrition ⇒ Colorectal disorders ⇒ Inflammatory bowel disease
2. A 27-year-old female presents to the emergency department with a 3-day history of a widespread painful rash. She reports having started a new medication for her seizures 1 week ago. On examination, you note erythematous macules that are coalescing into large areas of epidermal detachment. The mucous membranes of her mouth, eyes, and genital region are also affected, and the skin involvement covers more than 30% of her body surface area. A skin biopsy reveals full-thickness epidermal necrosis. Based on her presentation and the medication history, which of the following diagnoses is she most likely suffering from, and which medication most likely contributed to this condition?
A) Erythema multiforme major secondary to Levetiracetam (Keppra)
B) Toxic Epidermal Necrolysis (TEN) secondary to Carbamazepine
C) Stevens-Johnson syndrome (SJS) secondary to Metformin
D) Acute generalized exanthematous pustulosis secondary to Lisinopril
E) Stevens-Johnson syndrome (SJS) secondary to Atorvastatin
Answer and topic summary
The answer is B) Toxic Epidermal Necrolysis (TEN) secondary to Carbamazepine
The patient’s presentation with widespread epidermal necrosis, mucous membrane involvement, and skin detachment affecting more than 30% of her body surface area is suggestive of Toxic Epidermal Necrolysis (TEN). SJS and TEN are considered a spectrum of the same disease, with SJS affecting less than 10% of body surface area, SJS-TEN overlap affecting 10-30%, and TEN affecting more than 30%. The diagnosis can be confirmed by biopsy (showing necrotic epithelium) if clinical characteristics (eg, target lesions progressing to bullae, ocular and mucous membrane involvement, Nikolsky sign, desquamation in sheets) are inconclusive. Immediate discontinuation of the offending drug is paramount. Patients with TEN often require transfer to a burn unit or an intensive care unit for supportive care. Fluid and electrolyte balance, pain control, and prevention of secondary infections are critical. Immunomodulatory agents like IVIG (intravenous immunoglobulin) or cyclosporine may be considered, but their efficacy is still under debate.
Option A: Erythema multiforme major: Presents with targetoid lesions and is less severe than SJS and TEN. Levetiracetam is not strongly associated with SJS or TEN.
Option D: Acute generalized exanthematous pustulosis is an extensive formation of nonfollicular sterile pustules on erythematous background combined with fever and peripheral blood leukocytosis. This uncommon eruption is most often an allergic reaction because of drugs such as aminopenicillins and sulfonamides inter alia.
A good way to remember the body surface area affected in TEN is “T hree x T en = T hirty percent in Toxic Epidermal Necrolysis
The distinction between SJS, SJS/TEN overlap, and TEN is based on the type of lesions and the amount of the body surface area with blisters and erosions
- Blisters and erosions cover between 3% and 10% of the body in SJS
- 11–30% in SJS/TEN overlap
- over 30% in TEN
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Dermatology ⇒ Desquamation ⇒ Toxic epidermal necrolysis and Stevens-Johnson syndrome
3. A 32-year-old male presents to his primary care physician complaining of persistent fatigue, unintentional weight loss over the past 3 months, and a painless swelling in the left side of his neck. On examination, there is a non-tender, rubbery 3cm lymphadenopathy in the left cervical region. A subsequent excisional biopsy of the node is performed, and microscopy reveals large atypical cells with abundant cytoplasm and bilobed nuclei, reminiscent of an “owl’s eye” appearance. What is the most likely diagnosis?
A) Acute lymphoblastic leukemia (ALL)
B) Non-Hodgkin’s Lymphoma
C) Burkitt’s lymphoma
D) Hodgkin’s Lymphoma
E) Chronic lymphocytic leukemia (CLL)
Answer and topic summary
The answer is D) Hodgkin’s Lymphoma
The patient’s clinical presentation with painless cervical lymphadenopathy and constitutional symptoms, coupled with the histological finding of large cells bearing the “owl’s eye” appearance (Reed-Sternberg cells), is characteristic of Hodgkin’s Lymphoma. Hodkin’s lymphoma is the most common type of lymphoma and usually presents as a solitary cervical lymph node that has been there for > 30 days. It is commonly manifested with painless cervical adenopathy; there may be splenomegaly or enlargement of other immune tissue, fever, weight loss, fatigue, or night sweats. Upper body lymph nodes are the most common. Diagnosis is based on clinical presentation and confirmed by an excisional biopsy of an involved lymph node. Histology often reveals the pathognomonic Reed-Sternberg cells, which have bilobed nuclei. A chest radiograph should be obtained to search for mediastinal adenopathy. Treatment for Hodgkin’s Lymphoma depends on the stage of the disease and typically involves a combination of chemotherapy, most commonly the ABVD regimen (Adriamycin, Bleomycin, Vinblastine, Dacarbazine). Radiation therapy might be added, especially for localized disease.
Answer Choices Explanations:
A) Acute lymphoblastic leukemia (ALL): Affects mainly children and presents with bone marrow failure symptoms.
B) Non-Hodgkin’s Lymphoma: A group of lymphoid malignancies. Reed-Sternberg cells distinguish Hodgkin’s Lymphoma from Non-Hodgkin’s types.
C) Burkitt’s lymphoma: Fast-growing non-Hodgkin’s lymphoma linked to the Epstein-Barr virus. Exhibits a “starry sky” appearance on microscopy.
E) Chronic lymphocytic leukemia (CLL): A malignancy of mature B cells in older adults. Increased lymphocyte count and smudge cells on a peripheral blood smear.
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Hematology ⇒ Neoplasms, premalignancies, and malignancies ⇒ Lymphoma (ReelDx + Lecture)
4. A 65-year-old male presents to your office complaining of fatigue and shortness of breath with exertion. The patient reports minimal cough. On physical exam, you note a thin, barrel-chested man with decreased heart and breath sounds, pursed-lip breathing, end-expiratory wheezing, and scattered rhonchi. Chest X-ray reveals a flattened diaphragm, hyperinflation, and a small, thin-appearing heart. PFTs show a decreased FEV1 / FVC ratio.
A) Asthma
B) Chronic bronchitis
C) Emphysema
D) Pulmonary fibrosis
E) Bronchiectasis
Answer and topic summary
The answer is C. Emphysema
The patient’s presentation of shortness of breath with exertion, barrel-chested appearance, pursed-lip breathing, findings on chest X-ray (e.g., flattened diaphragm, hyperinflation, and a small heart), and pulmonary function test results all align with the diagnosis of emphysema.
Emphysema is a lung disease that causes shortness of breath. It is one of the two main conditions that make up chronic obstructive pulmonary disease (COPD). The other condition is chronic bronchitis.
In emphysema, the air sacs (alveoli) in the lungs are damaged. Over time, the inner walls of the air sacs weaken and rupture — creating larger air spaces instead of many small ones. This reduces the surface area of the lungs and, in turn, the amount of oxygen that reaches your bloodstream.
The main cause of emphysema is cigarette smoking. Other causes include air pollution and chemical fumes. A small percentage of cases are caused by a familial or genetic disorder, alpha-1-antitrypsin deficiency.
- The body’s natural response to ↓ lung function is chronic hyperventilation = Pink Puffers! CO2 Retainers – the body must increase ventilation to blow off CO2
- Minimal cough (compared to chronic bronchitis), quiet lungs
- Minimal sputum (compared to chronic bronchitis)
- Thin, underweight, and barrel chest
Answer Choices Explanations:
A) Asthma: An obstructive lung disease that is reversible and is marked by bronchoconstriction. It typically presents with episodes of wheezing triggered by factors such as allergens, exercise, or infections.
B) Chronic bronchitis: Defined by a productive cough for 3 consecutive months in 2 successive years. It’s a subtype of chronic obstructive pulmonary disease (COPD), with its main causative factor being smoking. The primary concern is mucus production, as opposed to the alveolar wall destruction seen in emphysema.
D) Pulmonary fibrosis: Represents a set of disorders causing scarring of the lung tissue, leading to a restrictive lung disease pattern. Symptoms might include a dry cough, finger clubbing, and inspiratory crackles upon examination.
E) Bronchiectasis: It is marked by the chronic dilation of bronchi or bronchioles due to repeated infections and inflammation. Patients often have a chronic cough and produce significant amounts of sputum.
Smarty PANCE Content Blueprint Review:
Covered under ⇒ PANCE Blueprint Pulmonary ⇒ Chronic obstructive pulmonary diseases ⇒ Emphysema
Also covered as part of the Internal Medicine EOR, Family Medicine EOR, and General Surgery EOR topic lists
5. A 68-year-old woman presents to the emergency department with chest pain that started 5 hours ago. She describes the pain as a heavy pressure radiating to her left arm. It began at rest and has persisted. She has a history of hypertension and diabetes mellitus. An ECG shows ST-segment depressions in leads II, III, and aVF. Troponin I levels are elevated at 0.55 ng/mL (normal: <0.04 ng/mL). Which of the following is the most likely diagnosis?
A) Stable angina
B) Unstable angina
C) Non-ST segment elevation myocardial infarction (NSTEMI)
D) ST-segment elevation myocardial infarction (STEMI)
E) Prinzmetal angina
Answer and topic summary
The answer is C) Non-ST segment elevation myocardial infarction (NSTEMI)
This patient’s presentation with chest pain at rest, ST-segment depressions on ECG, and elevated troponin I levels are consistent with NSTEMI. NSTEMI is characterized by myocardial ischemia severe enough to result in myocyte injury and elevated cardiac biomarkers but not sufficient to cause ST-segment elevation on ECG.
NSTEMI is diagnosed clinically with supporting findings from ECG changes, especially ST-segment depressions or T-wave inversions, and elevated cardiac biomarkers (troponins or CK-MB). Elevated troponins, in particular, differentiate NSTEMI from unstable angina.
Immediate management includes antiplatelet agents (e.g., aspirin, clopidogrel), anticoagulation (e.g., heparin or enoxaparin), and nitrates for symptom relief. A coronary angiography, followed by possible revascularization (percutaneous coronary intervention or coronary artery bypass grafting), might be required based on risk assessment.
Answer Choices Explanations:
A) Stable angina: Characterized by predictable chest pain or discomfort with exertion or stress, which is relieved by rest or nitroglycerin.
B) Unstable angina: Presents as chest pain at rest, new-onset angina, or angina that is more frequent, longer in duration, or not relieved by rest/nitroglycerin. Crucially, cardiac biomarkers (e.g., troponins) remain normal, differentiating it from NSTEMI.
D) ST-segment elevation myocardial infarction (STEMI): Acute myocardial infarction characterized by ST-segment elevation on ECG. Requires immediate reperfusion therapy.
E) Prinzmetal angina: Caused by coronary artery spasm leading to transient ST-segment elevation. Pain typically occurs at rest, often in the early morning hours.
Smarty PANCE Content Blueprint Review:
PANCE Blueprint Cardiology => Coronary Heart Disease (PEARLS) => Non-ST-Segment Elevation MI (NSTEMI) ReelDx
This podcast is available on every device!
You can download and listen to past FREE episodes here, on iTunes, Spotify, Google Podcasts, Stitcher, Amazon Music, and all podcasting apps.
Download Interactive Content Blueprint Checklists for the PANCE, PANRE, EOR, and PANRE-LA
Follow this link to download your FREE copy of the PANCE/PANRE/EOR Content Blueprint Checklists.
Print it up and start crossing out the topics you understand, marking the ones you don’t, and making notes of key terms you should remember. The PDF version is interactive and linked directly to the individual lessons on Smarty PANCE.
Smarty PANCE is not sponsored or endorsed by, or affiliated with, the National Commission on Certification of Physician Assistants.
The post Podcast Episode 107: This vs. That – PANCE Blueprint Comparisons You Need to Know (Part 1) appeared first on The Audio PANCE and PANRE.
68 episoder
Alle episoder
×Velkommen til Player FM!
Player FM scanner netter for høykvalitets podcaster som du kan nyte nå. Det er den beste podcastappen og fungerer på Android, iPhone og internett. Registrer deg for å synkronisere abonnement på flere enheter.
Lik The Audio PANCE and PANRE Physician Assistant Board Review Podcast
A top podcast for healthcare leaders, with over one million downloads, Radio Advisory is your weekly download on how to untangle the industry's most pressing challenges to help leaders like you make the best business decisions for your organization. From unpacking major trends in care delivery—like site-of-care shifts and the rise of high-cost drugs—to demystifying stakeholder dynamics, to shining a spotlight on priorities that may get overlooked, we're here to help. Our hosts and seasoned r ...
…
continue reading
Montgomery & Company (MoCo) is a weekly podcast and radio show hosted by two-time WNBA Champion and Co-Owner/Vice President of the Atlanta Dream, Renee Montgomery, in partnership with WABE Atlanta. Both insightful and compelling, MoCo features interviews with some of the world’s top athletes, entertainers, and innovators as well as roundtable discussions with Renee’s colleagues, friends, and family, about sports, culture and building generational wealth. Montgomery & Company: Sports, Cultu ...
…
continue reading
The Art of Charm is where self-motivated people, just like you, come to learn from the company’s coaches about to how to master human dynamics, relationships, and becoming your best self with the help of Johnny and AJ, the company’s founders. Johnny and AJ bring their 11 years of coaching experience from their famous Bootcamps, where they host clients in Los Angeles from all over the world and they share their stories, best practices and themselves on this weekly podcast. Not only does The A ...
…
continue reading
Join host and Harvard Business School Online Creative Director Chris Linnane as he sits down with HBS faculty to discuss business education in a way that’s both entertaining and insightful. The Parlor Room is your key to breaking down academic theory without sacrificing depth—all while gaining practical takeaways for navigating the business world.
…
continue reading
How can business help solve society’s biggest challenges? Welcome to Series 3 of Take on Tomorrow, the award-winning podcast from PwC that examines the biggest problems facing society and the role business can—and should—play in solving them. This series, we’re welcoming broadcaster and journalist Femi Oke to the show. She joins podcaster and journalist Lizzie O’Leary, and together with industry innovators, tech trailblazers and visionary leaders from around the globe, they’ll explore timely ...
…
continue reading
The traditional enterprise go-to-market motion is undergoing a transformational shift. B2B buyers are more sophisticated than ever, and operational efficiency is a key focus for every organization. One key function possesses a unique opportunity to shape the future of revenue generation: enablement. On this podcast, we’re bringing you the secrets, strategies, and tactics that successful enablement leaders are using to drive meaningful impact. The Enablement Edge is the go-to resource for sal ...
…
continue reading
AnthroPod is produced by the Society for Cultural Anthropology. In each episode, we explore what anthropology teaches us about the world and people around us.
…
continue reading
From the stuff your mother never told you, to the stuff your doctor never learned, On Health features taboo-busting conversations that demystify and de-stigmatize our bodies, all while bridging the gap between conventional medicine and wellness. Join Yale-trained MD & midwife Aviva Romm and her line-up of expert guests as they discuss everything from periods to menopause, sex to reproductive health politics, and motherhood to mental health. Each week, Dr. Romm will be exploring the science a ...
…
continue reading
New episode every Wednesday! Join the Barbell Shrugged crew in conversations about fitness, training, and frequent interviews w/ CrossFit Games athletes!
…
continue reading
I Tyngre Radio snackas det om styrketräning. Punkt. Värdar är Alex Danielsson och Andreas Guiance.
…
continue reading
Player FM - Podcast-app
Gå frakoblet med Player FM -appen!
Gå frakoblet med Player FM -appen!




{kind=link}